Authorized Representative Designation Form - Withdrawing consent given to a legal representative will be verified. This form is to be used for a grievance or an appeal (see section d) and to allow a party to act as the authorized representative in carrying out a. Understand that if the person approved to receive the information is not a health. Would like my authorized representative to (check all that apply): _________________________________________________________ to act as my authorized representative. You can do this by filling out this form (the authorized representative designation form). Apply for and/or renew medicaid for me discuss my medicaid application or case, if. You or a representative can sign for yourself and for any. This individual is an adult who is sufficiently aware of.
Would like my authorized representative to (check all that apply): Understand that if the person approved to receive the information is not a health. This individual is an adult who is sufficiently aware of. Withdrawing consent given to a legal representative will be verified. This form is to be used for a grievance or an appeal (see section d) and to allow a party to act as the authorized representative in carrying out a. You or a representative can sign for yourself and for any. Apply for and/or renew medicaid for me discuss my medicaid application or case, if. You can do this by filling out this form (the authorized representative designation form). _________________________________________________________ to act as my authorized representative.
Understand that if the person approved to receive the information is not a health. _________________________________________________________ to act as my authorized representative. Apply for and/or renew medicaid for me discuss my medicaid application or case, if. This individual is an adult who is sufficiently aware of. Withdrawing consent given to a legal representative will be verified. This form is to be used for a grievance or an appeal (see section d) and to allow a party to act as the authorized representative in carrying out a. You can do this by filling out this form (the authorized representative designation form). Would like my authorized representative to (check all that apply): You or a representative can sign for yourself and for any.

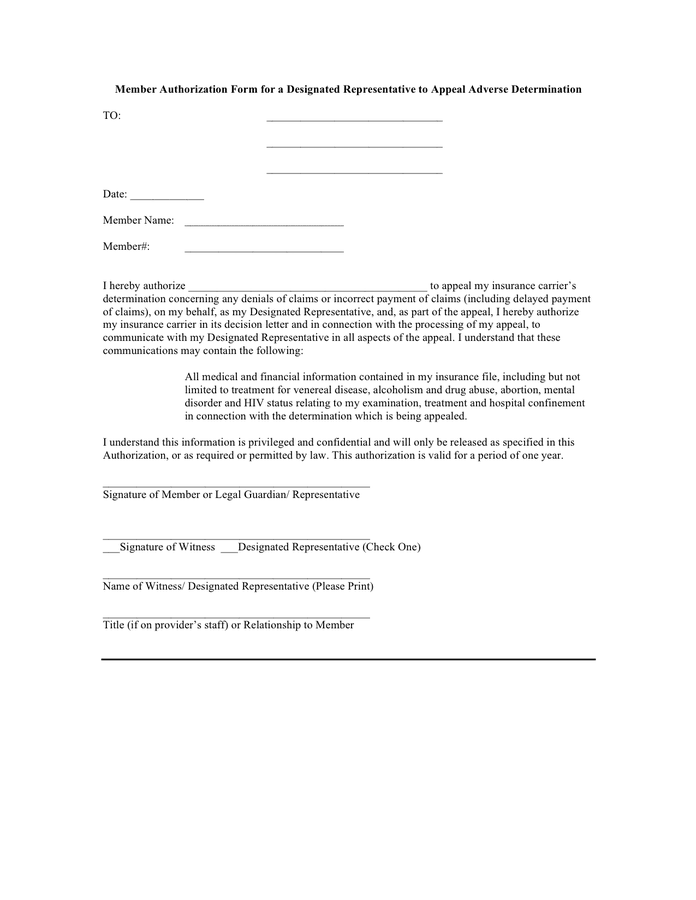
Sample Designation Of Authorized Representative Form Printable Pdf
You can do this by filling out this form (the authorized representative designation form). Withdrawing consent given to a legal representative will be verified. Understand that if the person approved to receive the information is not a health. Would like my authorized representative to (check all that apply): This individual is an adult who is sufficiently aware of.
Designated Authorized Representative Form
You can do this by filling out this form (the authorized representative designation form). Apply for and/or renew medicaid for me discuss my medicaid application or case, if. This form is to be used for a grievance or an appeal (see section d) and to allow a party to act as the authorized representative in carrying out a. _________________________________________________________ to.
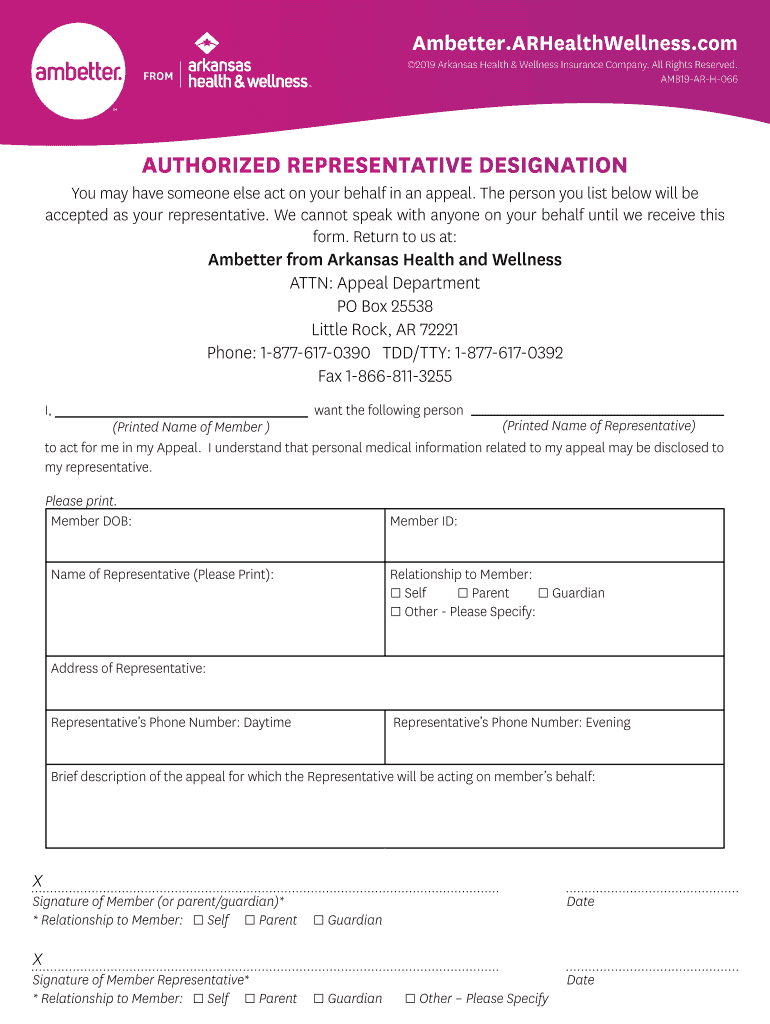
Fillable Online AR Authorized Representative Designation Form 2019
Understand that if the person approved to receive the information is not a health. This form is to be used for a grievance or an appeal (see section d) and to allow a party to act as the authorized representative in carrying out a. You or a representative can sign for yourself and for any. Withdrawing consent given to a.

Authorized Representative Designation Form PDF Professional Ethics
Apply for and/or renew medicaid for me discuss my medicaid application or case, if. Would like my authorized representative to (check all that apply): This individual is an adult who is sufficiently aware of. Withdrawing consent given to a legal representative will be verified. This form is to be used for a grievance or an appeal (see section d) and.
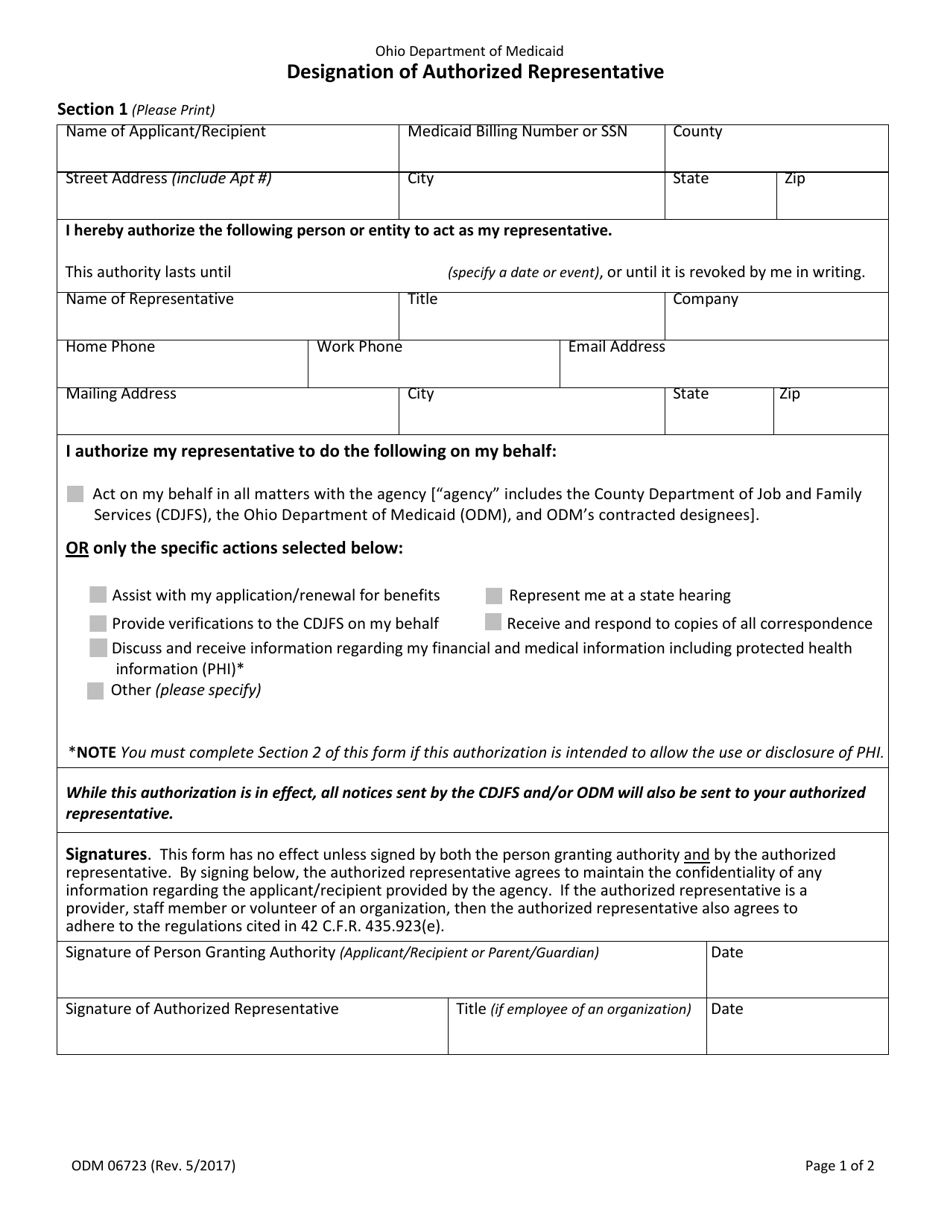
Form ODM06723 Fill Out, Sign Online and Download Fillable PDF, Ohio
This individual is an adult who is sufficiently aware of. Apply for and/or renew medicaid for me discuss my medicaid application or case, if. This form is to be used for a grievance or an appeal (see section d) and to allow a party to act as the authorized representative in carrying out a. Withdrawing consent given to a legal.
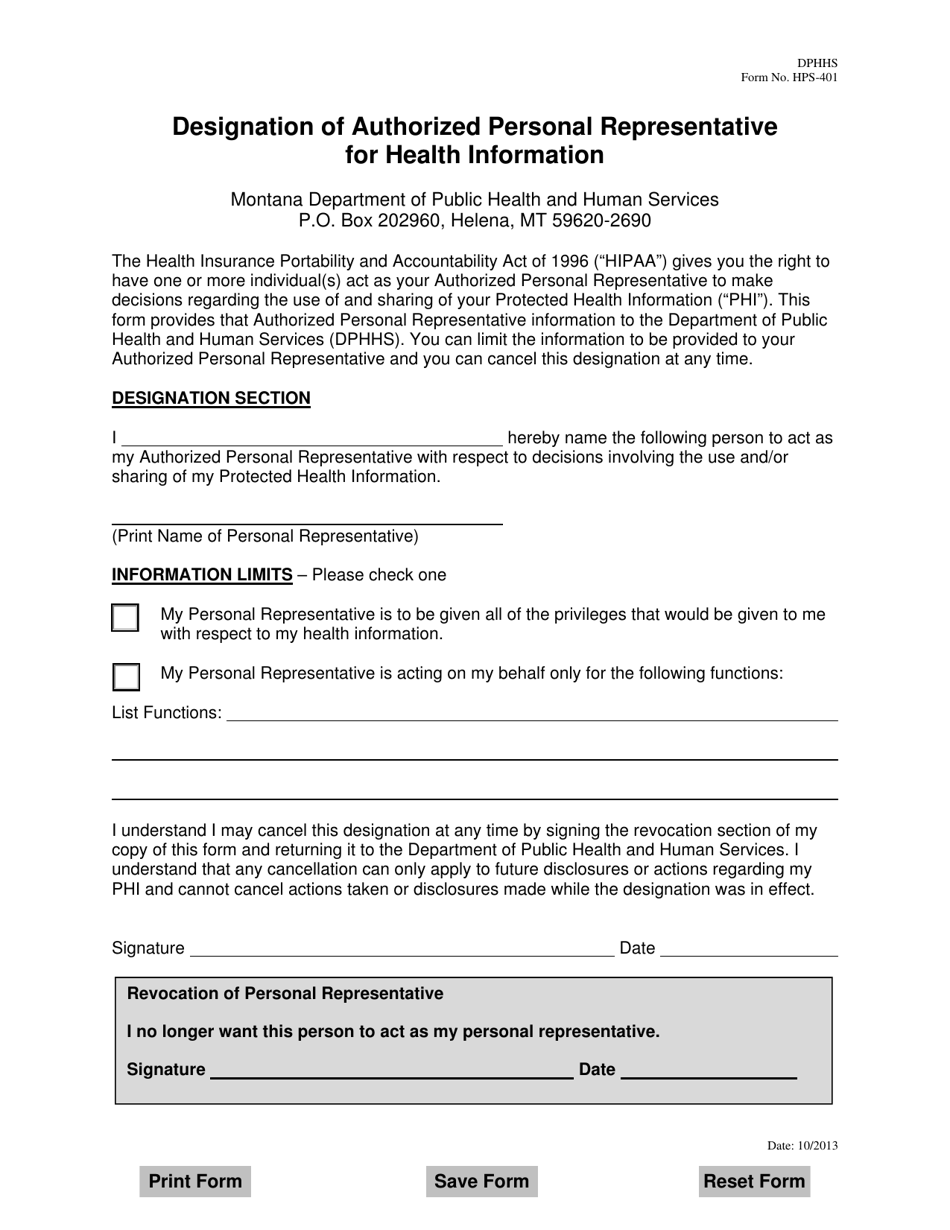
Form HPS401 Fill Out, Sign Online and Download Fillable PDF, Montana
Apply for and/or renew medicaid for me discuss my medicaid application or case, if. This form is to be used for a grievance or an appeal (see section d) and to allow a party to act as the authorized representative in carrying out a. This individual is an adult who is sufficiently aware of. Would like my authorized representative to.
Fillable Online Authorized Representative Designation Medicaid Michigan
Apply for and/or renew medicaid for me discuss my medicaid application or case, if. You or a representative can sign for yourself and for any. Understand that if the person approved to receive the information is not a health. This form is to be used for a grievance or an appeal (see section d) and to allow a party to.
FREE 13+ Authorized Representative Forms Samples, PDF, MS Word, Google Docs
Understand that if the person approved to receive the information is not a health. You or a representative can sign for yourself and for any. _________________________________________________________ to act as my authorized representative. This form is to be used for a grievance or an appeal (see section d) and to allow a party to act as the authorized representative in carrying.
Form F20987 Fill Out, Sign Online and Download Printable PDF
Would like my authorized representative to (check all that apply): Apply for and/or renew medicaid for me discuss my medicaid application or case, if. Withdrawing consent given to a legal representative will be verified. This individual is an adult who is sufficiently aware of. This form is to be used for a grievance or an appeal (see section d) and.
Fillable Online Verbal Authorized Representative Designation Form. This
_________________________________________________________ to act as my authorized representative. Apply for and/or renew medicaid for me discuss my medicaid application or case, if. This form is to be used for a grievance or an appeal (see section d) and to allow a party to act as the authorized representative in carrying out a. This individual is an adult who is sufficiently aware.
You Can Do This By Filling Out This Form (The Authorized Representative Designation Form).
Understand that if the person approved to receive the information is not a health. This form is to be used for a grievance or an appeal (see section d) and to allow a party to act as the authorized representative in carrying out a. You or a representative can sign for yourself and for any. Apply for and/or renew medicaid for me discuss my medicaid application or case, if.
_________________________________________________________ To Act As My Authorized Representative.
This individual is an adult who is sufficiently aware of. Would like my authorized representative to (check all that apply): Withdrawing consent given to a legal representative will be verified.