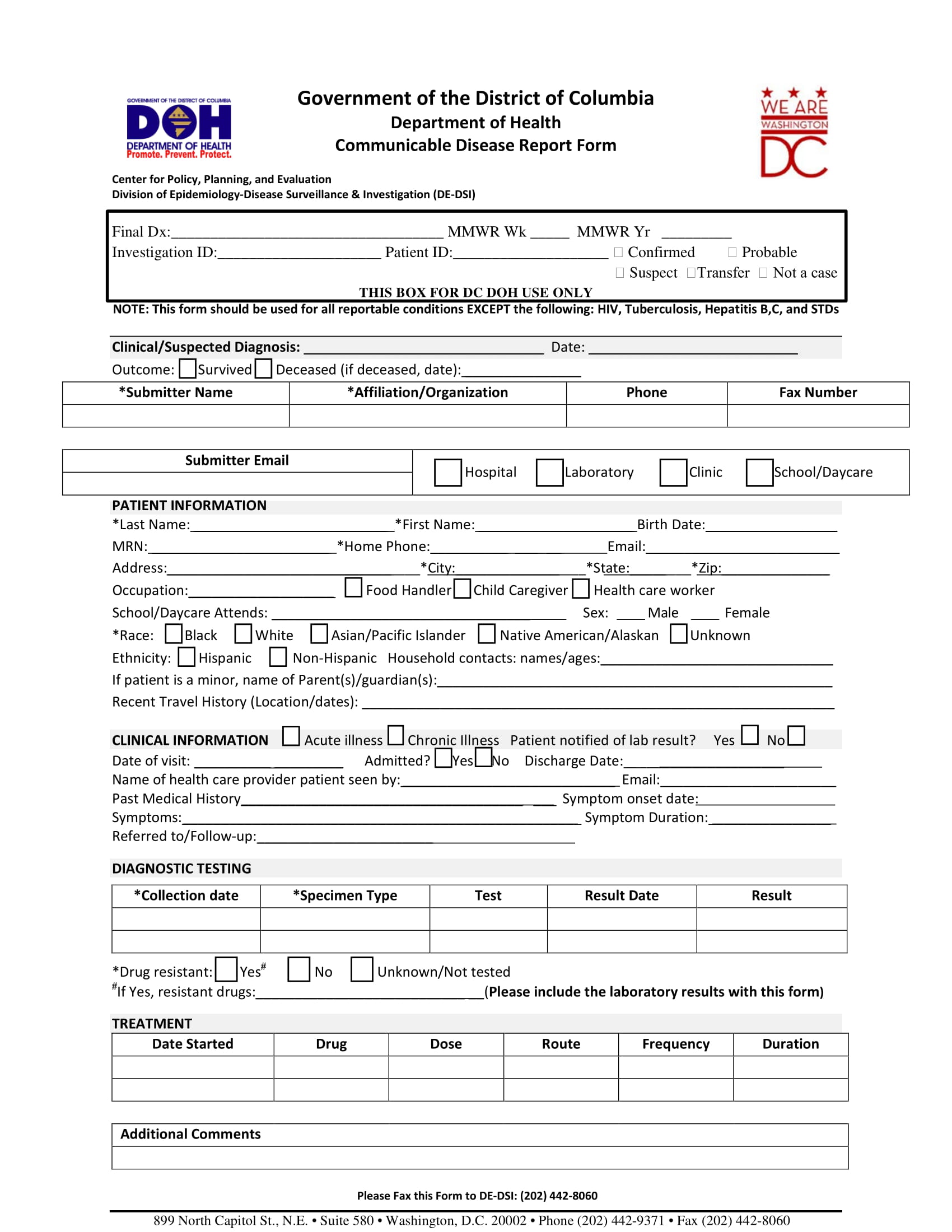
Free Of Communicable Disease Form - I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. Complete the following information to notify the florida department of health of a reportable disease or condition. Physician’s statement form date of physical: Statement of good health/free of communicable disease explanation and instruction: ________________ i have examined _______________________________________, and to. This 9 can be filled in electronically. Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that.
Complete the following information to notify the florida department of health of a reportable disease or condition. I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. Statement of good health/free of communicable disease explanation and instruction: This 9 can be filled in electronically. Physician’s statement form date of physical: Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. ________________ i have examined _______________________________________, and to.
This 9 can be filled in electronically. ________________ i have examined _______________________________________, and to. I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. Complete the following information to notify the florida department of health of a reportable disease or condition. Physician’s statement form date of physical: Statement of good health/free of communicable disease explanation and instruction: Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that.

Free of communicable disease form Fill out & sign online DocHub
This 9 can be filled in electronically. Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. Statement of good health/free of communicable disease explanation and instruction: I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental.
Fillable Online Free From Communicable Disease Statement Congregational
I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. This 9 can be filled in electronically. Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. ________________ i have examined _______________________________________,.
Alaska Confidential Infectious Disease Report Form Fill Out, Sign
I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. ________________ i have examined _______________________________________, and to. Complete the following information to.
Communicable Disease Screening Complete with ease airSlate SignNow
Physician’s statement form date of physical: I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. Complete the following information to notify the florida department of health of a reportable disease or condition. ________________ i have examined _______________________________________, and to. This 9 can be.

Fillable Online COMMUNICABLE DISEASE GUIDELINE CHART FOR CHILD CARE
I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. Complete the following information to notify the florida department of health of.

Free Of Communicable Disease Form Captions Trend Today
Physician’s statement form date of physical: Complete the following information to notify the florida department of health of a reportable disease or condition. ________________ i have examined _______________________________________, and to. Statement of good health/free of communicable disease explanation and instruction: Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no.
Fillable Online Division of Communicable Disease Control & Prevention
Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. Physician’s statement form date of physical: This 9 can be filled in electronically. Statement of good health/free of communicable disease explanation and instruction: I have examined the individual named above and to the best of my knowledge he/she.
FREE 15+ Case Report Forms in PDF MS Word
I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. Complete the following information to notify the florida department of health of a reportable disease or condition. Statement of good health/free of communicable disease explanation and instruction: ________________ i have examined _______________________________________, and to..
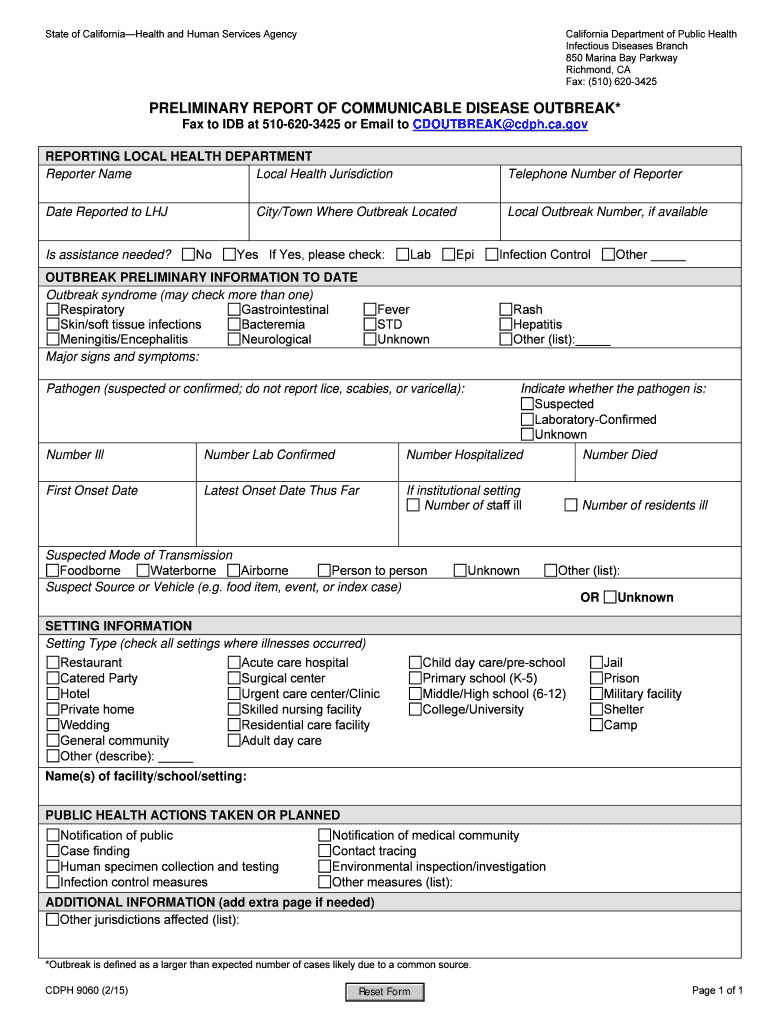
Fillable Online cdph ca Preliminary Report of Communicable Disease
I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. Complete the following information to notify the florida department of health of a reportable disease or condition. Physician’s statement form date of physical: Patient name and he/she (circle one) appears to be free of.
Communicable Disease Plan Template Doc Template pdfFiller
I have examined the individual named above and to the best of my knowledge he/she is in good physical and mental health, free of any communicable. Physician’s statement form date of physical: Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. Complete the following information to notify.
Statement Of Good Health/Free Of Communicable Disease Explanation And Instruction:
Complete the following information to notify the florida department of health of a reportable disease or condition. Physician’s statement form date of physical: Patient name and he/she (circle one) appears to be free of communicable diseases, including tuberculosis, and i have found no condition that. This 9 can be filled in electronically.
I Have Examined The Individual Named Above And To The Best Of My Knowledge He/She Is In Good Physical And Mental Health, Free Of Any Communicable.
________________ i have examined _______________________________________, and to.